Corona Virus
- Thread starter MTY
- Start date
-
Active since 1995, Hearth.com is THE place on the internet for free information and advice about wood stoves, pellet stoves and other energy saving equipment.
We strive to provide opinions, articles, discussions and history related to Hearth Products and in a more general sense, energy issues.
We promote the EFFICIENT, RESPONSIBLE, CLEAN and SAFE use of all fuels, whether renewable or fossil. -
Super Cedar firestarters 30% discount Use code Hearth2024 Click here
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
- Status
- Not open for further replies.
Henry Ford Health system has said it will ration access to ventilators based on the health of the patient, and their ability to survive the infection. Those deemed not able to recover will be made "comfortable".
Again not wanting to sound like a broken record or that the sky is falling but....... Conversations about DNR status with your loved ones are responsible right now. 3 levels basically. It's reasonable to talk about if/ how long you are willing to be machine dependant. Given the situation we are all entering, this is a conversation that allows family to know your wishes and theirs. Having to make a decision of taking someone off of machinery while not necessarily knowing their own words /wishes is horrible.
Again not wanting to sound like a broken record or that the sky is falling but....... Conversations about DNR status with your loved ones are responsible right now. 3 levels basically. It's reasonable to talk about if/ how long you are willing to be machine dependant. Given the situation we are all entering, this is a conversation that allows family to know your wishes and theirs. Having to make a decision of taking someone off of machinery while not necessarily knowing their own words /wishes is horrible.
I agree with having an advanced directive, it's a very smart thing to have. What's scary in this scenario from Henry Ford is a group of Dr's make the call, not you or your family. If you are deemed too unhealthy to survive, you will not get a ventilator, just medicine, I assume Morphine or something of that sort to make you comfortable.
Medic21
Minister of Fire
This is a last resort for triaging. It’s not a decision or situation we take lightly in the medical field. It also not you make and sleep well at night. Trust me I’ve had to do it in the field.I agree with having an advanced directive, it's a very smart thing to have. What's scary in this scenario from Henry Ford is a group of Dr's make the call, not you or your family. If you are deemed too unhealthy to survive, you will not get a ventilator, just medicine, I assume Morphine or something of that sort to make you comfortable.
If we allow two to die by caring for a lost cause while someone else dies from lesser injuries we failed all.
paulnlee
Feeling the Heat
This is a last resort for triaging. It’s not a decision or situation we take lightly in the medical field. It also not you make and sleep well at night. Trust me I’ve had to do it in the field.
If we allow two to die by caring for a lost cause while someone else dies from lesser injuries we failed all.
Yes, that is what they are saying, that this is a last resort, but it may come to this. I think it may help people stay home and heed the quarantine order our governor put in place. Up until now, people have been largely ignoring it.
Who was that nutty broad that mentioned "death panels"
This is not the same as a death panel, it doesn't matter if you have top of the line insurance or medicaid, this is simple math, we only have so may ventilators to go around. One Dr. figured out a way to hook one ventilator to two patients at once.
Henry Ford Health system has said it will ration access to ventilators based on the health of the patient, and their ability to survive the infection. Those deemed not able to recover will be made "comfortable".
Your reference is missing a lot of context. Its a contingency plan for what is hoped never happens. One the key tenet of disaster planning is look at every possibility in advance, make a rational plan in advance and hope it never happens. The short form is "fail to plan, plan to fail".
If someone wants the background on this, this link is going to supply background. https://www.clickondetroit.com/news...solute-worst-case-scenario-policy-not-active/
Its real easy to get caught up in the hype, if you just want to attract attention to yourself then keep on getting sucked in, on the other hand its not that hard to do your homework and actually contribute useful information to this thread.
Grizzerbear
Minister of Fire
Your reference is missing a lot of context. Its a contingency plan for what is hoped never happens. One the key tenet of disaster planning is look at every possibility in advance, make a rational plan in advance and hope it never happens. The short form is "fail to plan, plan to fail".
If someone wants the background on this, this link is going to supply background. https://www.clickondetroit.com/news...solute-worst-case-scenario-policy-not-active/
Its real easy to get caught up in the hype, if you just want to attract attention to yourself then keep on getting sucked in, on the other hand its not that hard to do your homework and actually contribute useful information to this thread.
Agreed.
(broken link removed to https://www-washingtonexaminer-com.cdn.ampproject.org/v/s/www.washingtonexaminer.com/news/assure-the-american-people-deborah-birx-condemns-reports-of-do-not-resuscitate-orders?amp_js_v=a3&
 sa=1&_amp=true&usqp=mq331AQFKAGwASA%3D#aoh=15853304893234&referrer=https%3A%2F%2Fwww.google.com&_tf=From%20%251%24s&share=https%3A%2F%2Fwww.washingtonexaminer.com%2Fnews%2Fassure-the-american-people-deborah-birx-condemns-reports-of-do-not-resuscitate-orders)
sa=1&_amp=true&usqp=mq331AQFKAGwASA%3D#aoh=15853304893234&referrer=https%3A%2F%2Fwww.google.com&_tf=From%20%251%24s&share=https%3A%2F%2Fwww.washingtonexaminer.com%2Fnews%2Fassure-the-american-people-deborah-birx-condemns-reports-of-do-not-resuscitate-orders)Yes, medicine and machinery can be a rabbit hole people enter unknowingly at times. I agree that there isn't a doctor on the planet that takes anything like this wilfully. Your hearing about a worst case scenario. Unfortunately it could truly happen in these times. Again what do you think your loved ones decision would reasonably be? Often the answer is obvious....me....I'm full resucitation, machinery for a 4 week maximum. My 75 year old dad with late stage Parkinson's disease, catheter, wheelchair and living in a nursing home he is basic resucitation with machinery for a week. Very basic conversation but brutal at the bedside. In November we were unprepared when my father was hospitalized and asked about feeding tubes. My dad was concious but delusional so the doctors made us answer the questions......talk about a moral gut ripping horrible position to be in ...even when the answer was somewhat obvious. He thankfully recovered and no feeding tube went in. Doing well (for him) at his nursing home today.
But even recalling the situation makes me want to puke.
But even recalling the situation makes me want to puke.
Your reference is missing a lot of context. Its a contingency plan for what is hoped never happens. One the key tenet of disaster planning is look at every possibility in advance, make a rational plan in advance and hope it never happens. The short form is "fail to plan, plan to fail".
If someone wants the background on this, this link is going to supply background. https://www.clickondetroit.com/news...solute-worst-case-scenario-policy-not-active/
Its real easy to get caught up in the hype, if you just want to attract attention to yourself then keep on getting sucked in, on the other hand its not that hard to do your homework and actually contribute useful information to this thread.
Why would I use something like this to draw attention to myself? What purpose would that serve? This was part of an internal document that was leaked. In retrospect, I should have just included the link. I'm not sure how things are where you live, but in the heavily populated greater Detroit area, they are spreading quickly.
Yes, medicine and machinery can be a rabbit hole people enter unknowingly at times. I agree that there isn't a doctor on the planet that takes anything like this wilfully. Your hearing about a worst case scenario. Unfortunately it could truly happen in these times. Again what do you think your loved ones decision would reasonably be? Often the answer is obvious....me....I'm full resucitation, machinery for a 4 week maximum. My 75 year old dad with late stage Parkinson's disease, catheter, wheelchair and living in a nursing home he is basic resucitation with machinery for a week. Very basic conversation but brutal at the bedside. In November we were unprepared when my father was hospitalized and asked about feeding tubes. My dad was concious but delusional so the doctors made us answer the questions......talk about a moral gut ripping horrible position to be in ...even when the answer was somewhat obvious. He thankfully recovered and no feeding tube went in. Doing well (for him) at his nursing home today.
But even recalling the situation makes me want to puke.
I hope I'm never put in that situation.
CaptSpiff
Minister of Fire
Medic21 was responding to a comment on the "leaked contingency plans of the Henry Ford Health System":
You are not understating that one bit!
I was a Volunteer Fire Fighter and responded to more car wrecks than I can recall. Two that stay with me were very bad multi-car scenes where only one ambulance responded. The Chief had to make the decision on who got to ride back and who had to wait. I saw the pain on his face and was glad those decisions weren't on me.
This is a last resort for triaging. It’s not a decision or situation we take lightly in the medical field. It also not you make and sleep well at night. Trust me I’ve had to do it in the field. Medic21
You are not understating that one bit!
I was a Volunteer Fire Fighter and responded to more car wrecks than I can recall. Two that stay with me were very bad multi-car scenes where only one ambulance responded. The Chief had to make the decision on who got to ride back and who had to wait. I saw the pain on his face and was glad those decisions weren't on me.
Medic21
Minister of Fire
are you saying I don’t understand it?Medic21 was responding to a comment on the "leaked contingency plans of the Henry Ford Health System":
You are not understating that one bit!
I was a Volunteer Fire Fighter and responded to more car wrecks than I can recall. Two that stay with me were very bad multi-car scenes where only one ambulance responded. The Chief had to make the decision on who got to ride back and who had to wait. I saw the pain on his face and was glad those decisions weren't on me.
move made the decision in combat of who got treated and who didn’t based in available supplies and personnel. Letting two Marines die that could have lived based on have a second medi vac and not just me. But could have is not a luxury in combat when two will if treated.
I’ve also had to leave people lay in a median to treat ones that were “salvageable” vs those that were alive yet with “injuries incomparable with life”.
So yes, I understand it. Still have the privilege of reliving those from time to time.
The leaked plans are the ugly truth of this situation now gets out of hand. It sucks and I hope it does not come to it.
kennyp2339
Minister of Fire
You are spot on!! I was alluding to this yesterday without saying it, unfortunately places like NYC are going to be the sacrificial lambs as far as aide, like the full compliment of ventilators, but the lesson learned in NYC will be great for places like Denver, Houston, Dallas ect...are you saying I don’t understand it?
move made the decision in combat of who got treated and who didn’t based in available supplies and personnel. Letting two Marines die that could have lived based on have a second medi vac and not just me. But could have is not a luxury in combat when two will if treated.
I’ve also had to leave people lay in a median to treat ones that were “salvageable” vs those that were alive yet with “injuries incomparable with life”.
So yes, I understand it. Still have the privilege of reliving those from time to time.
The leaked plans are the ugly truth of this situation now gets out of hand. It sucks and I hope it does not come to it.
are you saying I don’t understand it?
move made the decision in combat of who got treated and who didn’t based in available supplies and personnel. Letting two Marines die that could have lived based on have a second medi vac and not just me. But could have is not a luxury in combat when two will if treated.
I’ve also had to leave people lay in a median to treat ones that were “salvageable” vs those that were alive yet with “injuries incomparable with life”.
So yes, I understand it. Still have the privilege of reliving those from time to time.
The leaked plans are the ugly truth of this situation now gets out of hand. It sucks and I hope it does not come to it.
I'm not sure who he was referring to either. I thought it was me??
CaptSpiff
Minister of Fire
are you saying I don’t understand it?
I'm envisioning you channeling Joe Pesci in Goodfellas.
You are not understating that one bit!
My statement (above) focused on the depth and truth of what you said, and then reinforced it with a similar experience of my own; except mine was once removed. Feel free to re-read the post. And keep doing what you're doing, you are the true Tip of the Spear.

CaptSpiff
Minister of Fire
I have a friend in NYC (Manhattan) who lives in a pretty posh apartment building with a doorman. In chatting with the doorman she learned almost half the building is now empty, most having "gotten outta town". People of means have options.
I know it's rude to quote one's own post, but now it's getting serious out there:
Rhode Island's Governor directs State Police to pull over NY drivers?!?
In my best German accent: YOUR PAPERS PLEASE ?

ACLU Questions If Rhode Island State Police Can Stop New York Drivers
Travelers coming from New York will be required to self-quarantine for 14 days upon arriving in Rhode Island, Gov. Gina Raimondo announced Thursday.
 boston.cbslocal.com
boston.cbslocal.com
AlbergSteve
Minister of Fire
Sorry Kenny, there will be many more sacrificial lambs.You are spot on!! I was alluding to this yesterday without saying it, unfortunately places like NYC are going to be the sacrificial lambs as far as aide, like the full compliment of ventilators, but the lesson learned in NYC will be great for places like Denver, Houston, Dallas ect...
It's not just the severity. It is the unpreparedness that is concerning. This is compounded by those lowlifes that seek to mine this horrible situation to their own benefit.I am deeply worried for the u.s.a.
I have family living there. The severity is much greater than the people have been led to believe.
Death squads made real. Another reason to have a national health care system.Henry Ford Health system has said it will ration access to ventilators based on the health of the patient, and their ability to survive the infection. Those deemed not able to recover will be made "comfortable".
The reasons are known. CDC budgets cut. CDC pandemic response team cut. Advance CDC epidemiologist in China, cut. Stock piles of masks, ventilators, cut. Just in time supply chains sound good when one wants to maximize efficiency and profit, but that model doesn't fit for health care. The lesson being learned is that we need to take healthcare as seriously as national defense (which has lots of stockpiles of things it will never use).All these measures are necessary. The scary part is they are many weeks behind. The U.S. has taken the slow approach in comparison for reasons unknown.
Reading comprehension folks. Spiff said understating, not understanding.
Ashful
Minister of Fire
This is likely one of the primary vectors for spreading the disease to new areas, over the last week. When you look at the estimated infection rates for NYC, there’s no doubt some of those people fleeing NYC into the surrounding states of NJ, PA, and CT have carried the virus with them.I have a friend in NYC (Manhattan) who lives in a pretty posh apartment building with a doorman. In chatting with the doorman she learned almost half the building is now empty, most having "gotten outta town". People of means have options. Probably second homes in your bedroom communities.
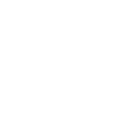
Hopefully it doesn’t come to this. Begreen actually posted the proper response to this post a week ago, but here’s a more simplified graphic demonstrating the same point:Henry Ford Health system has said it will ration access to ventilators based on the health of the patient, and their ability to survive the infection. Those deemed not able to recover will be made "comfortable".
![[Hearth.com] Corona Virus](https://www.hearth.com/talk/data/attachments/258/258746-26ad96e37554f0168c1295f75eee4062.jpg?hash=yzTA9wd9R_ "[Hearth.com] Corona Virus")
Note the area under the curve, or the total number of people infected, is the same. Social distancing is aimed at limiting the rate of the spread to a threshold below which our hospitals can handle the critical cases, not the total count of people who get this thing. However, due to seasonal factors and continued research on possible treatments, delaying the spread will likely also decrease the number of critical cases ending in death.
Good! I wish PA were doing the same. People are supposed to stay put, not carry this thing around the country with them.Rhode Island's Governor directs State Police to pull over NY drivers?!?
In my best German accent: YOUR PAPERS PLEASE ?
There are too many variables to say there “will” be anything.Sorry Kenny, there will be many more sacrificial lambs.
Lol... was wondering if someone was going to catch that. Still, the misunderstanding generated an interesting response.Reading comprehension folks. Spiff said understating, not understanding.
You’re absolutely blinded and insane if you think the government could take complete control and run healthcare.
I would think it can be done as many/most countries do it currently. It's under funded is the case in general. Here in our city (10th biggest in the country) it's not a matter of space, the hospital has lots of room, it's a matter of staff and equipment. I completely understand the magnitude of the problems of where the reasonable line is set, but this is approaching shameful that all countries don't have supplies ready and waiting for high volume situations. I'm hoping that won't ever happen again.
I’m waiting for the government to deploy the combat support hospital. That would be a quick way to add to our healthcare industry with the active duty military personnel and have the level two trauma center capabilities. They can handle the majority of the day today for larger cities to allow them to focus their facilities on COVID-19
The Military is stationing the Hospital ship Mercy off the port of LA, and the Hospital ship Comfort off the coast of New York. Trump also said he was ordering the Army Corps of Engineers to build make shift ICU's.
- Status
- Not open for further replies.